Hyperbaric oxygen therapy (HBOT) is defined as the use of oxygen at higher than atmospheric pressure for the treatment of underlying disease processes and the diseases they produce. Modern HBOT in which 100% O2 is breathed in a pressurized chamber dates back to the 1930s, when it was first used for treatment of decompression illness in divers. There are currently 13 FDA-approved uses for HBOT, including decompression illness, gas gangrene, air embolism, osteomyelitis, radiation necrosis, and the most recent addition—diabetic ulcers. HBOT can dramatically and permanently improve symptoms of chronic TBI months or even many years after the original head injury. This assertion is generally met with skepticism within the medical establishment because we have been taught for generations that any post-concussion symptoms persisting more than 6 months or so after a head injury are due to permanent brain damage that cannot be repaired.
The National Brain Injury Rescue and Rehabilitation Project was established as a preliminary study to test the safety and practicality of multi-center hyperbaric oxygen administration for the post-concussive symptoms of chronic mild traumatic brain injury as a precursor to a pivotal, independent, multi-center, controlled clinical trial. This report presents the results for 32 subjects who completed a preliminary trial of hyperbaric oxygen several years before the passage of the 21 st Century Cures Act. This study anticipated the Act and its reassessment of clinical research. Subjects received 40-82 one-hour treatments at 1.5 atmospheres absolute 100% oxygen. Outcome measures included repeated self-assessment measures and automated neurocognitive tests. The subjects demonstrated improvement in 21 of 25 neurocognitive test measures observed. The objective neurocognitive test components showed improvement in 13 of 17 measures. Earlier administration of hyperbaric oxygen post injury, younger age at the time of injury and hyperbaric oxygen administration, military status, and increased number of hyperbaric oxygen administrations were characteristics associated with improved outcomes. There were no adverse events. Hyperbaric oxygen was found to be safe, inexpensive and worthy of clinical application in the 21 st Century model of facile data collection provided by recent research regulatory shifts in medicine. The study was approved by the ethics review committee of the Western Institutional Review Board (WIRB; Protocol #20090761).
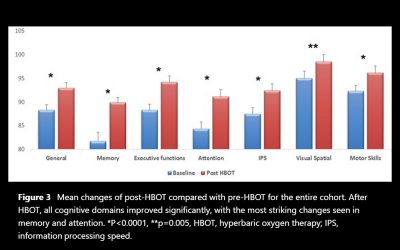
The aim of the study is to evaluate the effect of hyperbaric oxygen therapy (HBOT) in participants suffering from chronic neurological deficits due to traumatic brain injury (TBI) of all severities in the largest cohort evaluated so far with objective cognitive function tests and metabolic brain imaging. A retrospective analysis was conducted of 154 patients suffering from chronic neurocognitive damage due to TBI, who had undergone computerised cognitive evaluations pre-HBOT and post-HBOT treatment. The average age was 42.7-14.6 years, and 58.4% were men. All patients had documented TBI 0.3-33 years (mean 4.6-5.8, median 2.75 years) prior to HBOT. HBOT was associated with significant improvement in all of the cognitive domains, with a mean change in global cognitive scores of 4.6-8.5 (p<0.00001).
This report is a product of the VA Evidence-based Synthesis Program. The purpose is to provide “timely and accurate syntheses of targeted healthcare topics. to improve the health and healthcare of Veterans”. The authors have made a comprehensive search and analysis of the literature and make recommendations to assist clinicians in dealing with veterans suffering from either traumatic brain injury (TBI) or post-traumatic stress disorder (PTSD). The report is timely and of great potential impact given the vigorous and lengthy debate among hyperbaric physicians and lay people determined to find an answer for the large numbers of veterans deeply affected with some combination of PTSD and post-concussion dysfunction.
Hyperbaric oxygen therapy (HBOT) serves as primary or adjunctive therapy for a diverse range of medical conditions. The indication for HBOT can be related to either pressure (decompression sickness or air emboli) or tissue hypoxia. It is now realized, that the combined action of hyperoxia and hyperbaric pressure, leads to significant improvement in tissue oxygenation while targeting both oxygen and pressure sensitive genes, resulting in improved mitochondrial metabolism with anti-apoptotic and anti-inflammatory effects. Clinical studies published in recent year’s present convincing evidence that HBOT can be the coveted neurotherapeutic method for brain repair. Here we discuss the multi-faceted role of HBOT in wound care in general and in neurotherapeutics in detail.
Present study evaluates the neuroprotective effect of β-elemene alone and in combination with hyperbaric oxygen (HO) in traumatic brain injury (TBI). TBI was induced by dropping a weight from a specific height. All the animals were separated in to five groups (n=20) like control group; TBI group; β-elemene treated group which receives β-elemene (100 mg/kg, i.p.) half an hour after the injury; HO group which receives hyperbaric oxygen therapy and β-elemene + HO group which receives β-elemene (100 mg/kg, i.p.) half an hour after the injury and hyperbaric oxygen therapy. Neurological function was assessed to evaluate the effect of β-elemene in TBI rats. Thereafter level of inflammatory cytokines and expression of protein of inflammatory pathway was assessed in the brain tissues of TBI rats.
To investigate the effect of hyperbaric oxygen therapy (HBOT) on traumatic brain injury (TBI) outcome. The modified Marmarou’s weight drop device was used to generate non-lethal moderate TBI rat model, and further developed in vitro astrocytes culturing system. Then, we analyzed the expression changes of interested genes and protein by quantitative PCR and western blot. Multiple HBO treatments significantly reduced the expression of apoptosis promoting genes, such as c-fos, c-jun, Bax and weakened the activation of Caspase-3 in model rats. On the contrary, HBOT alleviated the decrease of anti-apoptosis gene Bcl-2 and promoted the expression of neurotrophic factors (NTFs), such as NGF, BDNF, GDNF and NT-3 in vivo. As a consequent, the neuropathogenesis was remarkably relied with HBOT.
Mild traumatic brain injury (TBI) persistent post-concussion syndrome (PPCS) and post-traumatic stress disorder (PTSD) are epidemic in United States Iraq and Afghanistan War veterans. Treatment of the combined diagnoses is limited. The aim of this study is to assess safety, feasibility, and effectiveness of hyperbaric oxygen treatments (HBOT) for mild TBI PPCS and PTSD. Thirty military subjects aged 18-65 with PPCS with or without PTSD and from one or more blast-induced mild-moderate traumatic brain injuries that were a minimum of 1 year old and occurred after 9/11/2001 were studied. The measures included symptom lists, physical exam, neuropsychological and psychological testing on 29 subjects (1 dropout) and SPECT brain imaging pre and post HBOT.
There has been no major advancement in a quarter of a century for the treatment of acute severe traumatic brain injury (TBI). This review summarizes 40 years of clinical and pre-clinical research on the treatment of acute TBI with hyperbaric oxygen therapy (HBO2) in the context of an impending National Institute of Neurologic Disorders and Stroke (NINDS)-funded, multicenter, randomized, adaptive Phase II clinical trial – the Hyperbaric Oxygen Brain Injury Treatment (HOBIT) trial. Thirty studies (8 clinical and 22 pre-clinical) that administered HBO2 within 30 days of a TBI were identified from PubMed searches. The pre-clinical studies consistently reported positive treatment effects across a variety of outcome measures with almost no safety concerns, thus providing strong proof-of-concept evidence for treating severe TBI in the acute setting.
Hyperbaric oxygen (HBO) therapy and neural stem cell (NSC) transplantation can improve traumatic brain injury (TBI) clinically. This study aimed to investigate the mechanism of HBO promoting NSC proliferation and neurological recovery after TBI. Twenty-four Sprague-Dawley rats were divided randomly into three groups: a sham group, a TBI group (constructed using Feeney’s free-fall method), and an HBO-treated TBI group. Neurological function was evaluated by Neurological Severity Scores on days 1, 3, and 7, and we found that TBI-induced poor neurological function was improved by HBO. On day 7 after TBI, we observed that TBI promoted NSC proliferation, migration to the lesion area, and the levels of vascular endothelial growth factor (VEGF), VEGFR2, Raf-1, MEK1/2, and phospho-extracellular signal-regulated kinase (ERK) 1/2 protein, which were further boosted by HBO, from immunohistochemistry, immunofluorescence, and Western blot experiments. In vitro, cell injury was applied to NSCs isolated from neonatal Sprague-Dawley rats by the Cell Injury Controller II system. Moreover, data from the BrdU Kit and Western blot showed that in-vitro HBO significantly accelerated NSC proliferation and the levels of proteins related to cell cycle and the VEGF/ERK pathway after cell injury, which was suppressed by the VEGFR2 inhibitor. Taken together, this study indicated that HBO may promote NSC proliferation by activating VEGF/ERK signaling and play a crucial role in neuroprotection after TBI.